
You just got your annual blood results back. Cholesterol checked. Blood sugar checked. Homocysteine nowhere on the panel. Again. Maybe you read that homocysteine affects heart disease and brain health. So you’re wondering: did your doctor miss something? Or is there a reason this test keeps getting left out?
Skipping it is usually intentional, and the science behind that decision is more solid than you might think. But there are real situations where you should ask for this test. This article breaks down what homocysteine is, why routine labs skip it after 50, when testing actually makes sense, and what to do if your levels come back high. No medical degree needed.
What Is Homocysteine — and Why Should You Care?
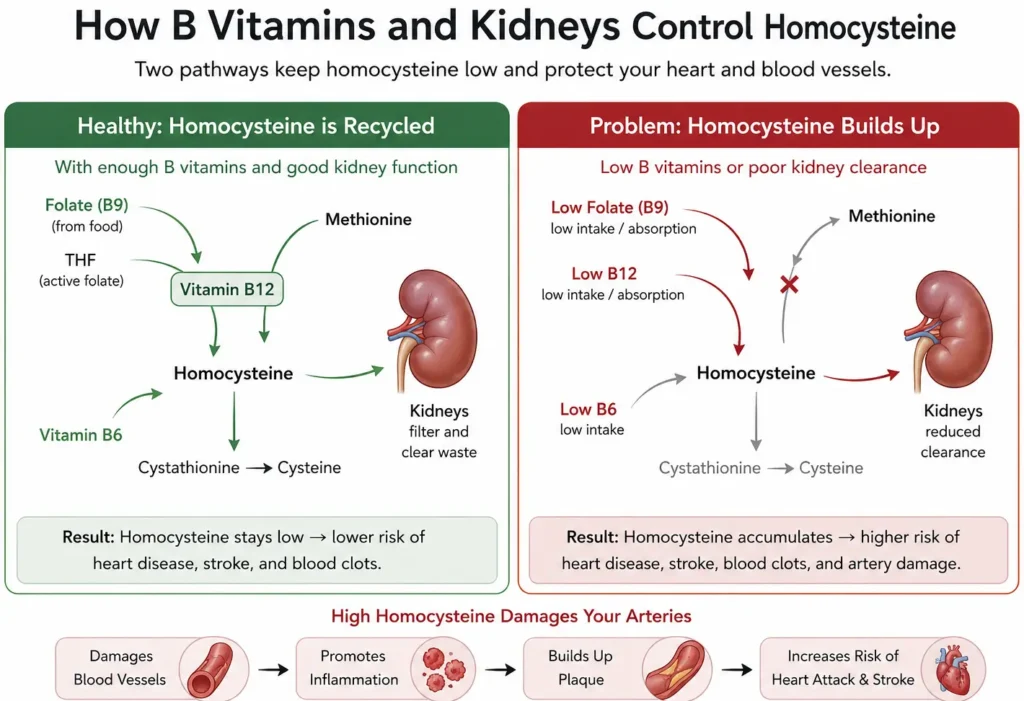
Think of homocysteine like exhaust from an engine. Every time your body breaks down protein from food, such as meat, eggs, and dairy, it produces homocysteine as a byproduct.
In a healthy body, that exhaust gets recycled quickly. Your body uses B vitamins, specifically B12, folate (B9), and B6, to convert homocysteine back into useful compounds.
So only tiny amounts stay in your blood. When those B vitamins are low, or when your kidneys can’t clear homocysteine fast enough, it builds up.
And that’s where problems can start. High homocysteine is linked to artery wall damage, blood clots, cognitive decline, and increased risk of stroke.
A large review found that every 5 µmol/L increase in homocysteine is associated with roughly a 22% higher risk of coronary heart disease. That’s a meaningful number. Normal levels for adults sit below 15 µmol/L. Mild elevation is 15,30.
Moderate is 30,100. Above 100 is rare and usually tied to a genetic condition. So if your number is slightly above 15, it doesn’t mean disaster, but it does mean something worth looking into.
Why Your Doctor Probably Didn’t Order This Test?
Here’s what surprises most people. Doctors aren’t skipping this test out of carelessness. It’s a deliberate choice backed by years of clinical trial data.
The American Heart Association does not recommend routine homocysteine screening for healthy adults. Why? Large randomized trials found that lowering homocysteine with B vitamins did not reliably reduce heart attacks or strokes in the general population.

That was the critical finding that changed everything. The 2024 AHA and American Stroke Association guidelines on stroke prevention, endorsed by the American Academy of Neurology and other major groups, made zero mention of homocysteine testing. That’s not an oversight. That’s a policy decision.
Insurance companies follow the same logic. Major insurers, including Blue Cross Blue Shield plans and Medicare Advantage, classify homocysteine as not medically necessary for general cardiovascular screening. Meaning they likely won’t pay for it if there’s no specific clinical reason.
And here’s the core problem with testing everyone: a high result tells you that something is off, not why. You’d still need to follow up with B12, folate, kidney function, and possibly genetic testing. One number, multiple possible causes. That’s not a useful screening tool for the general population.
What Aging Does to Your Homocysteine Levels?
Before you worry about a slightly elevated number, here’s what getting older actually does to this marker. After age 50, homocysteine levels rise naturally. Two main reasons drive this. First, kidney function declines gradually with age, and kidneys play a key role in clearing homocysteine from the blood.
Second, your stomach produces less acid as you age, which makes it harder to absorb B12 from food, and lower B12 means higher homocysteine.
For women, menopause adds another layer. Estrogen helps keep homocysteine in check. After menopause, levels often rise to match or exceed those of men the same age.
Research puts the average homocysteine for adults around age 65 at roughly 16.5 µmol/L, which is technically above the normal cutoff. And data from the Framingham Heart Study found that more than 40% of adults aged 80 and older had elevated homocysteine.
So if your result comes back at 17 or 18 µmol/L and you’re 62 years old, that may simply reflect the biology of aging. Mild elevation is common. It still deserves attention, but it isn’t automatically a red flag.
When Your Doctor SHOULD Order This Test
There are clear situations where skipping this test would be the wrong call. Here’s who should actually be tested. You have symptoms of B12 or folate deficiency. Homocysteine rises before B12 levels even show as low on standard tests. So it can catch a deficiency early.
Symptoms to watch for: unexplained fatigue, tingling in your hands or feet, memory problems, trouble with balance, or mood changes.
You have chronic kidney disease. Impaired kidneys can’t clear homocysteine efficiently. If you’ve been told your kidney function is reduced or if your GFR is declining, this test gives your doctor useful context.

You had a heart attack or stroke before age 55. Or if a first-degree relative (parent, sibling) did. Premature cardiovascular disease without obvious risk factors like smoking or high cholesterol warrants a deeper look.
You eat a plant-based diet. Vegans and vegetarians are at higher risk of B12 deficiency because B12 comes mainly from animal products. Without supplementation, homocysteine often climbs quietly.
Your doctor is evaluating you for cognitive decline. High homocysteine is linked to brain atrophy and increased Alzheimer’s risk. Some physicians include it in a cognitive health workup.
A 2025 review published in PMC confirms testing is appropriate for nutritional assessment in anemia or malabsorption cases, in chronic kidney disease, and in certain cardiovascular workups.
What to Do If Your Levels Come Back High?
A high result is a signal to investigate, not a verdict on your health. The first step is finding out why it’s elevated. Your doctor should follow up with a B12 test, a folate test, a B6 check, and a kidney function panel. If those come back normal, an MTHFR gene test may be the next step.
MTHFR is a common genetic variant, affecting up to 40% of people, that impairs how your body processes folate. If B12 deficiency is the cause, supplementation usually works well. Levels often improve within three to six months of consistent supplementation. Your doctor should retest to confirm the response.
If kidney disease is driving it, the homocysteine number is secondary. Treating the underlying kidney condition takes priority.
Diet plays a supporting role regardless of cause. Dark leafy greens boost folate. Eggs, fish, and meat support B12. Poultry and legumes help with B6. These aren’t cures on their own, but they create better conditions for your body’s recycling process to work.

Should You Ask Your Doctor for This Test? Use This Checklist
Go through these questions honestly. If two or more apply, bring them up at your next appointment with your specific symptoms in hand.
- Do you have unexplained fatigue, tingling, or memory lapses?
- Have you eaten a mostly plant-based diet for years without supplementing B12?
- Has your doctor flagged reduced kidney function or a low GFR?
- Did you or a close family member have a heart attack or stroke before age 55?
- Have you previously tested low for B12 or folate?
- Are you being evaluated for cognitive decline or early dementia signs?

If yes to two or more: bring it up specifically. Don’t just ask for more tests. Tell your doctor which symptoms you’re experiencing and why you want to explore homocysteine as part of the picture.
You can also order this test independently in most U.S. states through services like Personalabs or Quest Diagnostics without a doctor’s visit. But getting a high result on your own still requires follow-up with a provider who can interpret it in context.
Conclusion
Skipping homocysteine on a routine blood panel is medically sound for most healthy adults over 50. But if you have real symptoms, kidney disease, or early heart risk, it’s a test worth requesting. Know your reasons before you ask. The good news is that most causes of high homocysteine are fixable.
A B12 deficiency caught early responds well to supplements. A folate gap closes with diet changes. These are not scary problems. They are solvable ones, but only if you know how to look.
⚠️MEDICAL DISCLAIMER
This article is for informational purposes only. It does not replace medical advice, diagnosis, or treatment. The information covers homocysteine levels, B vitamins (B12, folate/B9, B6), cardiovascular risk, stroke prevention, aging and kidney function, post-menopause hormonal shifts, B12 or folate deficiency symptoms, plant-based diet risks, cognitive decline, supplementation, and dietary sources of B vitamins.
Individual results vary based on age, health status, and fitness level. Before changing your exercise routine, diet, or supplement use, talk to your doctor or a qualified health professional first. If you experience chest pain, dizziness, severe joint pain, or any sudden symptom during or after exercise, stop immediately and seek medical care.


