
You’re not falling apart. Women in their early 40s to early 50s are walking out of doctor’s offices with diagnoses of depression or anxiety when the real cause is a hormonal shift that the standard screening tools were never built to detect.
This article will not tell you that perimenopause mood changes misdiagnosed as mental illness is rare. It will show you exactly why it keeps happening, what the biology actually looks like, and what you can say at your next appointment to change the outcome.
| # | Section | What You’ll Find |
|---|---|---|
| 1 | The Broken Screening Tool | Why the test itself is part of the problem |
| 2 | What Hormones Do to Your Brain | The chemical chain no one explains to you |
| 3 | The Symptoms That Get Mislabeled | Why the mood clues look like something else |
| 4 | Getting a Better Diagnosis | What the right clinical conversation sounds like |
| 5 | Treatment That Fits the Cause | What changes when the diagnosis is correct |
| 6 | How to Stop the Misdiagnosis | Steps to take before your next appointment |
The Screening Tool That Was Not Built for You
You fill out a quick questionnaire at the doctor’s office and a few minutes later you have a diagnosis. That questionnaire may be quietly working against you. This is one of the clearest reasons why perimenopause mood changes misdiagnosed as depression keeps happening to women who are otherwise physically healthy.
Nearly four in 10 women seeking care for perimenopause symptoms have reported feeling misdiagnosed, according to a 2025 national survey of more than 1,000 women commissioned by Biote.¹
The tool doctors most commonly use to screen for depression is the PHQ-8 [a standardized eight-item questionnaire used to detect depressive symptoms in a general adult population].
Its eight items cover sleep disruption, fatigue, low interest in activities, concentration problems, appetite changes, low mood, self-critical thoughts, and psychomotor changes [feeling slowed down or restless].
Here is the structural problem. Seven of those eight items can be caused by perimenopause alone, and not by clinical depression.¹ Sleep disruption, fatigue, concentration problems, appetite changes, and mood disturbance are all documented perimenopause symptoms.
When a woman in the middle of a hormonal transition fills out this form, the score can point to clinical depression even when her brain chemistry is being destabilized by estrogen fluctuations, not by a mental health condition.
That same 2025 survey found that 33% of respondents received treatment for anxiety, 27% for depression, and 13% for panic attacks during this period.¹ Among women who were prescribed medication for a mental health condition during perimenopause, more than one-third believed they were not correctly diagnosed.¹
It is not a bad screening tool. It does what it was designed to do. The problem is that it was designed for a general adult population, and it was not built to separate hormonal mood instability from a primary psychiatric diagnosis.
What the questionnaire cannot see is what is happening inside the brain during a hormonal shift, and that is where the story actually starts.
Why Your Hormones Scramble the Mood Signals in Your Brain
You may have noticed that your mood can shift within the same day, and that no obvious external event triggered it. That is not a personal failing. That is a chemistry problem. The depression screening tool most doctors use in a quick office visit has seven of its eight questions answered “yes” by perimenopause itself, which means the tool cannot tell the difference between a hormonal shift and a mental health condition.

Here is what is actually happening. Estrogen is not just a reproductive hormone.
Estrogen receptors [specialized proteins in brain tissue that bind to estrogen and activate mood-regulating processes] are present in multiple brain regions involved in mood and cognitive regulation.² Estrogen also modulates the transmission of serotonin and noradrenaline, two chemicals the brain uses to maintain emotional stability.²
During perimenopause, estrogen and progesterone do not simply decline. They lurch.²˒³ Levels spike and drop in ways the brain has not experienced before.
Research has found that these erratic fluctuations in estradiol [the main form of estrogen active in the body] can disrupt serotonin, dopamine [a chemical linked to motivation and reward], and norepinephrine [a chemical involved in stress response and alertness], and are associated with mood instability, cognitive changes, and sleep disruption.³
The brain’s mood-regulating systems are sensitive to these swings, not just to a final low level of estrogen. This matters because it explains why some perimenopausal women feel fine for a week and then feel completely unlike themselves for three days with no warning. The problem is not a stable, low hormone level. It is unpredictability.
The fluctuation is the trigger. That distinction is important for treatment, and it is covered in Section 5.
The Perimenopause Mood Changes Most Often Misdiagnosed
You’ve probably described these feelings to someone and heard “it’s just stress.” It is not just stress, and you are far from alone in hearing that.
Approximately 70% of women experience some form of emotional disturbance during perimenopause, including irritability, anxiety, and depressive symptoms.⁴
There is actually a clinical name for what you are experiencing. The American College of Obstetricians and Gynecologists has named a specific pattern called perimenopausal mood instability [a recognized clinical term for the mood changes that arise from hormonal fluctuations during the transition to menopause, distinct from a diagnosis of clinical depression].⁵
This is not a synonym for depression. It has its own characteristics.

What makes it hard to catch:
- The mood changes may arrive with no pattern relative to the menstrual cycle
- They can last years, not days
- They include irritability that comes out of nowhere, sudden crying without a clear reason, and a feeling women consistently describe as “not feeling like myself”
- They do not always respond to antidepressants the same way that a primary depressive disorder does
The numbers confirm what many women already feel. A 2024 meta-analysis of seven studies involving 9,141 women across five countries found that perimenopausal women were around 40% more likely to experience depressive symptoms than premenopausal women.⁶
That increase in risk is real. But a higher risk of depressive symptoms is not the same as a confirmed diagnosis of clinical depression that exists independently of hormonal change.
The piece that gets lost is that for a large group of women, the depressive symptoms are downstream of the hormonal disruption. Address the hormonal disruption and the mood picture can change significantly.
Knowing what it is called is the first step. Knowing what to do with that information at your next appointment is what the next section covers.

Symptom Checklist: Clues That Point Toward Perimenopause Rather Than Primary Depression
Talk to your doctor before changing any existing medication or starting new treatment if you are managing a chronic condition, take daily prescription drugs, or are uncertain about your hormone status.
- Mood changes that started around the same time your cycle became irregular
- Irritability or anger that arrives suddenly and fades quickly, with no external cause
- Good days and bad days with no pattern you can predict
- Sleep disruption that arrived at the same time as mood changes
- Anxiety or low mood that does not match your typical mental health history
- Prior treatment for depression that is no longer working the way it used to
What a Correct Diagnostic Conversation Actually Sounds Like
Most women have to start this conversation themselves. Only 42% of clinicians initiated discussion about perimenopause in care settings, and only 15% of women felt adequately informed when their symptoms began, according to the same 2025 survey.¹
A separate report found that 25% of women aged 50 to 65 had never been told by their doctor that they were in perimenopause or menopause, even though 92% of those same women had experienced at least one related symptom in the past year.⁷
That gap is not your fault. It is a gap in how perimenopause has historically been covered in medical training. But until that changes, the conversation has to start with you.

What to bring to your appointment:
A written record of when your mood changes started relative to any changes in your menstrual cycle. Doctors who understand perimenopause will look for this timing relationship. If your mood changed at the same time your periods became irregular, that is clinical information.
What to say directly:
“I’d like to discuss whether my mood symptoms could be connected to perimenopause before we settle on a mental health diagnosis.”
What to ask them to rule out:
Thyroid dysfunction mimics perimenopause mood symptoms closely, including fatigue, depression, and anxiety. Requesting a thyroid panel before accepting a mood disorder diagnosis is a reasonable step.
Published guidelines for evaluating perimenopausal depression emphasize ruling out alternative medical causes of mood symptoms through differential diagnosis. Because thyroid dysfunction can produce fatigue, depression, anxiety, and other symptoms that overlap with perimenopause, thyroid function testing is commonly considered during evaluation.⁸

If your current provider does not engage with the hormonal context of your symptoms, The Menopause Society maintains a searchable directory of certified menopause practitioners at menopause.org. These providers have passed a specialized examination in midlife women’s health and accept new patients.
The right question to ask is not “do I have depression?” It is “do I have depression, or does this look like hormonal mood instability, or both?”
Treatment That Matches the Real Cause
Being offered an antidepressant is not the wrong answer. It may be part of the right answer. But for women whose mood symptoms are being driven by hormonal fluctuations, an antidepressant that targets serotonin alone may not reach the actual source of the problem.
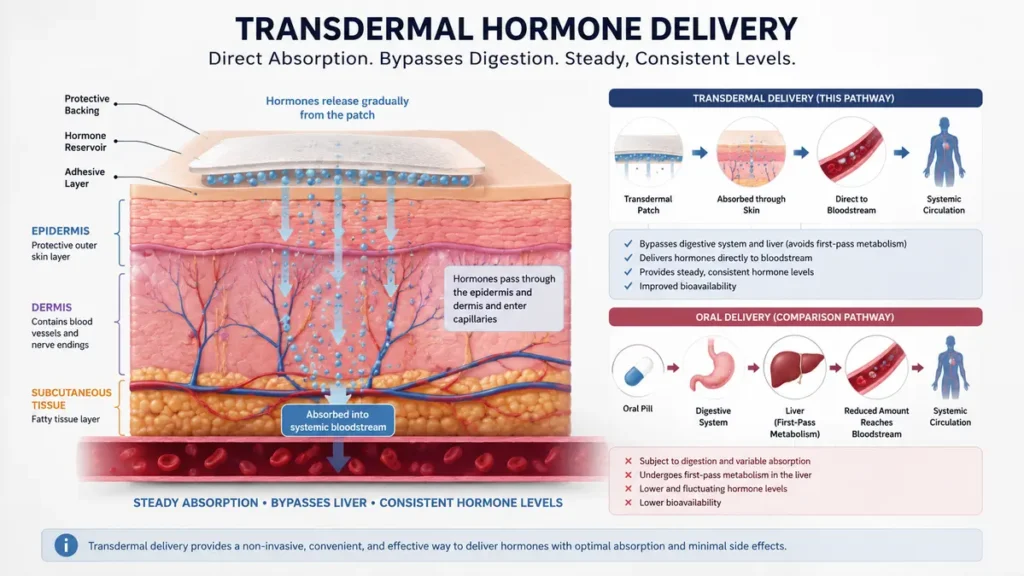
The NIH StatPearls clinical reference chapter on menopause, updated in 2026, states that evidence supports transdermal estrogen [estrogen delivered through the skin via patch or gel, bypassing the digestive system] for managing mood symptoms during the perimenopausal period.²
A 2025 peer-reviewed case report published in Cureus and indexed in PubMed found that two women with perimenopausal mood disorders, one aged 48 and one aged 55, saw marked mood improvement when transdermal estradiol [the bioactive form of estrogen] was added to their treatment plans after antidepressants alone had not produced adequate results.⁹
This does not mean hormone therapy is the right choice for every woman. It is not. Clinical decision-making in this area is individual and depends on medical history, contraindications, and symptom profile. The point is that hormone therapy is a recognized evidence-supported option that is not always offered when it could be.
Cognitive behavioral therapy, commonly known as CBT [a structured form of talk therapy that addresses specific thought patterns and behaviors], also has evidence behind it for perimenopausal mood symptoms, anxiety, hot flashes, and night sweats.¹⁰ It is a non-hormonal option worth discussing with your provider.
Published clinical guidelines on perimenopausal depression recommend that providers identify the menopausal stage, assess co-occurring menopause symptoms and psychosocial contributors, and consider all appropriate treatment options based on an individual woman’s clinical presentation.⁸
The goal is a treatment that matches the actual cause. If you do not know the cause yet, you are not in a position to evaluate whether the treatment is right.
How to Stop the Misdiagnosis Before It Happens
You are more prepared for this appointment than you think. The steps below work because they give your doctor clinical information they need to distinguish perimenopause mood instability from a primary psychiatric diagnosis.
Before your appointment:
- Track your mood changes for two to four weeks. Note the day, the intensity on a simple scale, and whether your cycle was regular or irregular that week
- Write down when your mood symptoms started and whether that timing overlapped with any change in your period
- List every current diagnosis and medication so your doctor can see the full picture

At your appointment:
- Open with: “My mood has been significantly different and I want to understand whether perimenopause could be a factor before we discuss a mental health diagnosis”
- Ask whether thyroid function has been assessed recently
- Ask whether a perimenopausal hormone assessment is appropriate given your age and the timing of your symptoms
If your provider does not engage with the hormonal context:
- Ask for a referral to a specialist
- Search the Menopause Society certified practitioner directory at menopause.org using your ZIP code
- Telehealth options are available through certified practitioners if local access is limited
The data makes one thing clear: this is not a rare problem, and the system is not yet designed to catch it reliably.¹ That is why the step forward falls to you for now.
Ask your doctor specifically whether your mood symptoms might be tied to perimenopausal hormone changes before accepting a mental health diagnosis alone. That one question, asked directly, is the most effective thing you can do with the information in this article.
Conclusion
The single most important step you can take today is to name the possibility out loud in your next medical appointment.
Ask your doctor specifically whether your mood symptoms might be tied to perimenopausal hormone changes before accepting a mental health diagnosis alone. The screening tools most offices use were not designed to separate hormonal mood instability from clinical depression, and that gap is fixable once you know it exists.
You now know it exists, and naming perimenopause mood changes misdiagnosed as depression for what it is, a system failure rather than a personal one, starts with you.
⚠️DISCLAIMER:
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The content addresses perimenopausal mood changes and misdiagnosis in clinical settings and is intended for general educational purposes only. Health conditions vary significantly between individuals, always consult a licensed physician or qualified healthcare provider before making any decisions about your health or medical care.
References
- Perimenopause misdiagnosis affects nearly 40% of women as clinicians fail to recognize hormonal transition. Patient Care Online. 2025. https://www.patientcareonline.com/view/perimenopause-misdiagnosis-affects-nearly-40-of-women-as-clinicians-fail-to-recognize-hormonal-transition
- Menopause. StatPearls. National Center for Biotechnology Information, NIH. Updated 2026. https://www.ncbi.nlm.nih.gov/books/NBK507826/
- Deshpande N, Sathyanarayana Rao TS. Psychological changes at menopause: anxiety, mood swings, and sexual health in the biopsychosocial context. SAGE Open Medicine. 2025. https://journals.sagepub.com/doi/10.1177/26318318251324577
- Han Y et al. Mitochondrial dysfunction in perimenopausal mood disorders: from hormonal shifts to neuroenergetic failure (review). PMC. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12513434/
- Mood changes during perimenopause are real. American College of Obstetricians and Gynecologists. https://www.acog.org/womens-health/experts-and-stories/the-latest/mood-changes-during-perimenopause-are-real-heres-what-to-know
- Women are 40% more likely to experience depression during the perimenopause. UCL News, citing Journal of Affective Disorders meta-analysis of 9,141 women. 2024. https://www.ucl.ac.uk/news/2024/may/women-are-40-more-likely-experience-depression-during-perimenopause
- In the misdiagnosis of menopause, what needs to change? AJMC contributor piece. 2025. https://www.ajmc.com/view/contributor-in-the-misdiagnosis-of-menopause-what-needs-to-change-
- Maki PM et al. Guidelines for the evaluation and treatment of perimenopausal depression: summary and recommendations. Menopause. 2018. https://pubmed.ncbi.nlm.nih.gov/30182804/
- Mogallapu R et al. Beyond selective serotonin reuptake inhibitor (SSRIs): exploring hormonal therapy for mood disorders in perimenopause and postmenopause. Cureus. 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12619688/
- National Institute for Health and Care Excellence (NICE). Cognitive Behavioural Therapy. Menopause: Evidence Review A. NICE Guideline No. 23. 2024. https://www.ncbi.nlm.nih.gov/books/NBK609725/


