
You wake up after eight hours of sleep and feel like you did not sleep at all. By noon the weight behind your eyes is already familiar. You push through it, because you have been told, sometimes gently, sometimes impatiently, that this is simply what getting older feels like for women past 55. That explanation is doing a lot of heavy lifting for a lot of suffering.
Persistent fatigue in women over 55 is not an inevitable feature of aging: it is one of four specific, treatable medical conditions that standard clinical screening routinely fails to catch. The problem is not your body giving up.
The problem is that the tests being ordered, and the numbers being read, were never built to find what is actually wrong.
Why read this:
- Find out why a ferritin result that prints “within normal limits” can still mean your iron stores are too low to sustain basic energy
- Learn which thyroid number doctors read as reassuring but researchers now question as a diagnostic gap
- Discover why sleep apnea looks nothing like snoring in women, and why that keeps it undiagnosed for years
- Understand what late-life depression actually looks like in women, and why exhaustion, not sadness, is often the only visible sign
- Get a concrete list of what to ask your doctor to test, and why most standard panels miss all four causes
Why the Standard Doctor Visit Is Built to Miss What Is Making You This Tired
You walk in, you describe bone-deep exhaustion, and you leave with your thyroid marked “normal,” your blood count flagged as fine, and a pamphlet about sleep hygiene. Nothing found. Nothing changed. That experience is not a one-off failure. It is the predictable result of how standard screening was designed.

The fatigue that affects women past 55 is not random. Research tracking middle-aged and older women found that 67.9% of postmenopausal women report clinically significant fatigue, a rate meaningfully higher than in women who have not yet gone through menopause.¹
In a separate cross-sectional study of 300 women across stages of menopause, 85.3% of postmenopausal women reported physical and mental exhaustion, compared with 19.7% of premenopausal women.²
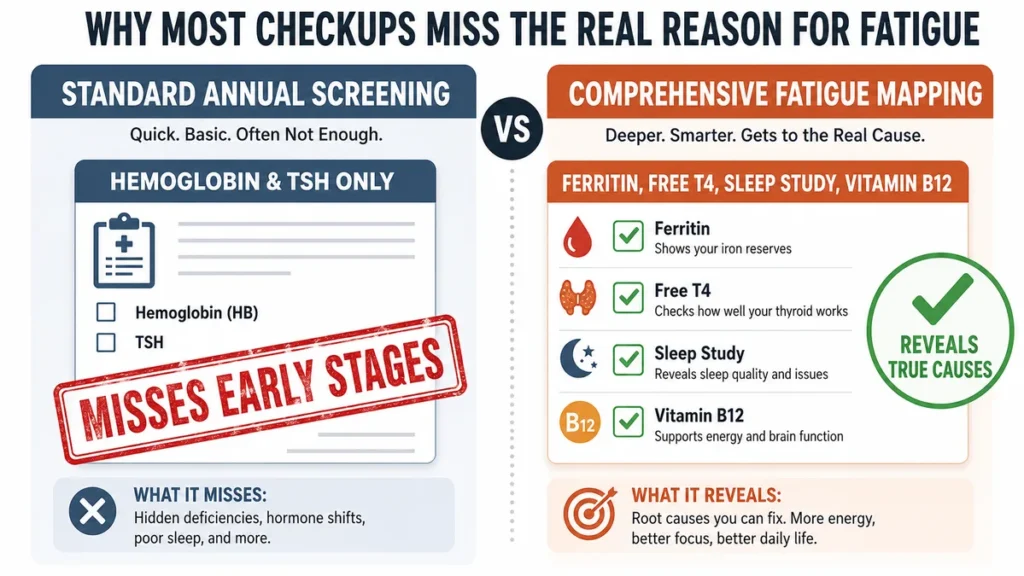
The gap is this large. And yet the standard annual panel most women receive tests for anemia using hemoglobin alone, which catches only the most advanced stage of iron deficiency.
It reads a thyroid number without accounting for the range of values where symptoms appear. It does not include a sleep disorder screening. It does not look for depression presenting as exhaustion rather than sadness.
Every cause covered in this article involves a diagnostic failure, not a biological inevitability. No single study has tested all four conditions together in women past 55; the case for each is built from separate research, each targeting one piece.
The condition is real. The detection gap is real. That distinction is what this article is about.
Fatigue in women over 55 is not a complaint to manage. It is a signal that something specific can be found and treated.
The Iron Test That Prints “Normal” While Your Stores Are Low Enough to Cause Exhaustion
Your blood work comes back and nothing is flagged. What you may not know is that the reference range your lab used to define “normal” was not designed to tell you whether your iron stores are high enough to sustain energy.
It was designed to tell you whether you have full anemia. Those are not the same question.
Iron deficiency without anemia [having iron stores too low to support normal cell function even though hemoglobin remains above the anemia threshold] is a distinct condition.
A randomized controlled trial of non-anaemic women with unexplained fatigue found that oral iron supplementation reduced fatigue scores by 29% in the iron group compared to 13% in the placebo group, with the benefit concentrated entirely in women whose ferritin was at or below 50 micrograms per liter.³
Your ferritin number can sit inside the lab’s printed “normal” range while your iron stores are low enough to fuel exhaustion, hair loss, and mood changes, because the standard cutoff of 12 to 15 ng/mL was set by expert opinion in 1993 and has not been updated to reflect what research shows about when symptoms actually begin.⁵

The symptoms start well before the number the lab flags as deficient.
A physiologically based analysis published in Blood in 2025 identified a ferritin threshold of 33 micrograms per liter for postmenopausal women using the point at which hemoglobin begins to fall as the marker, more than double the current WHO guideline of 15.⁵
A 2023 paper published in the American Society of Hematology Education Program made the case directly: 30% to 50% of healthy women show no iron in bone marrow stores despite having ferritin values still within the lab’s normal range.¹³
The medicine has moved. The lab reference range has not.
That is not a minor administrative gap. If your ferritin has ever come back “within normal limits” while you are exhausted, it is worth asking your doctor which cutoff was used to read it.
The Thyroid Number That Looks Fine on Paper While Your Energy Collapses
You feel cold in rooms where everyone else is comfortable. You have put on weight without a meaningful change in what you eat. Your hair is thinner than it was two years ago.

Your doctor runs a thyroid panel, the result falls inside the reference range, and you are told the thyroid is not the problem.
It may still be the problem. It just may not be showing up the way the test was designed to catch it.
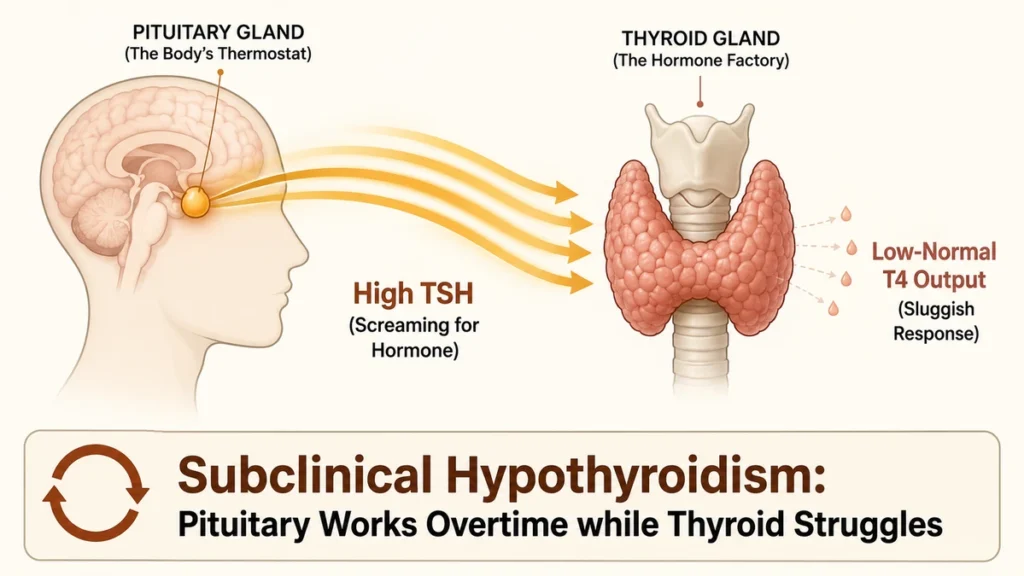
Subclinical hypothyroidism [a condition where the thyroid-stimulating hormone, which tells the thyroid gland to produce more hormone, is elevated, but the thyroid hormone levels in the blood still fall within normal range] sits in a diagnostic gray zone.
A cross-sectional study of 142 postmenopausal women aged 45 to 70 identified subclinical hypothyroidism in 22.5% of participants, with the condition most common in women within five to ten years of menopause.⁶
Here is the direct challenge to what you have probably been told: having a TSH result that falls within the normal range does not mean your thyroid is contributing nothing to your fatigue. The diagnostic system has a structural bias toward catching overt disease.
A nested study within a randomized, placebo-controlled trial found that giving levothyroxine to older adults with mild subclinical hypothyroidism produced no measurable improvement in physical or mental fatigue.⁷
This matters, not because it proves the thyroid is irrelevant, but because it means “your TSH is fine” and “your thyroid is not causing your fatigue” are answering different questions.
Thyroid symptoms in women over 55 overlap closely with the symptoms of iron deficiency, sleep apnea, and depression. Each condition on this list produces fatigue, cold intolerance, mood changes, and cognitive slowing. No single test clears all four at once.
The approach that catches the cause is a panel, not a single number.
The Sleep Disorder That Does Not Look Like Snoring in Women
You do not snore loudly. You do not wake up gasping. You wake up after a full night and feel like you never slept. You fall asleep in the early afternoon. You have headaches in the morning.
You are moody in a way you cannot explain. Your doctor, working from a mental model of sleep apnea as a condition that heavy men get, does not send you for a sleep study.
Obstructive sleep apnea [a sleep disorder in which the airway repeatedly narrows or closes during sleep, interrupting breathing and pulling the sleeper out of deep rest without fully waking them] presents differently in women than in men.
Female patients with obstructive sleep apnea are significantly more likely to report insomnia, depressive symptoms, fatigue, morning headache, and nightmares rather than the hallmark loud snoring that most clinicians and patients associate with the condition.⁸

The prevalence numbers are striking. Research has found that sleep apnea in women increases substantially following menopause, with studies identifying obstructive sleep apnea in 47% to 67% of postmenopausal women.⁹
Women with sleep apnea often have their symptoms attributed to menopause itself: the night sweats, the broken sleep, the daytime fatigue.
Because menopausal symptoms and sleep apnea symptoms overlap almost exactly, the sleep disorder can remain undiagnosed for years while the cause is being managed as a hormone problem.
One published review of gender issues in obstructive sleep apnea reported that women’s non-specific presentation, including lack of energy, fatigue, and mood disturbance, likely contributes directly to underdiagnosis and delay in diagnosis relative to men.⁸
The standard OSA screening checklist was built around the male presentation.
If you snore and you are overweight and you are a man, you get referred for a sleep study. If you are a postmenopausal woman who is tired and irritable and waking at 3 a.m., you may be told to reduce caffeine.
Ask your doctor specifically about obstructive sleep apnea if you are a postmenopausal woman with unexplained fatigue and disrupted sleep, even if you do not snore.
When Exhaustion Is Depression and Your Doctor Is Looking for Sadness Instead
You are not crying. You do not feel hopeless. You feel flat. You feel heavy. Getting out of bed takes more than it used to, and not because you are sad, but because you are tired in a way that sleep does not fix.

If your doctor is screening for depression using sadness as the primary indicator, this version of it will be missed.
The National Institute of Mental Health states that depression in older adults is frequently undiagnosed or misdiagnosed because sadness is not always the main symptom.¹⁰ In this age group, physical manifestations, including exhaustion, aches, cognitive slowing, and loss of motivation, are often more prominent than emotional ones.
Late-life depression [a depressive disorder occurring in adults over 60 that often presents with physical symptoms rather than obvious sadness, making it harder to identify through standard screening tools designed for younger patients] is a clinical category, not a softened version of the condition. It is depression. It requires treatment.
The evidence connecting fatigue and depression in older adults is genuinely complex.
A study of community-dwelling older adults found that interleukin-6, a marker of low-level inflammation, was linked to fatigue and to symptoms that mimic depression, especially apathy (loss of motivation), suggesting that inflammation may be a common thread connecting exhaustion and mood changes in later life.¹¹
Most of the direct evidence on depression and fatigue in this population comes from mixed-sex samples, and the research specifically isolating fatigue in women over 55 as a depression presentation remains limited. This is the honest state of the evidence.
What is clear is that exhaustion is one of the recognized symptoms of depression in older adults, and it is one of the least likely to trigger a mental health referral on its own.
Depression that presents primarily as fatigue is not a mild or sub-threshold version. It is underidentified. The treatment options are the same as for any other presentation.
What to Ask for at Your Next Appointment: A Testing Map You Can Bring In
You can leave your next appointment with answers rather than reassurances. The tests that cover all four conditions covered in this article exist, are accessible, and require only one thing: asking for them by name.
Four conditions produce the fatigue in women over 55 that standard screening misses. Each has a specific test:
Talk to your doctor before adding any supplement to your routine, especially if you are pregnant, on medication, or managing a chronic condition.
- Ferritin (not hemoglobin alone). Ask specifically for a ferritin level. If it comes back between 15 and 50 micrograms per liter,⁴ ask your doctor whether that result would fall below the symptomatic threshold identified in recent research. A result printed as “normal” may not mean your iron stores are adequate.
- TSH with free T4. A TSH result alone may not be sufficient if subclinical hypothyroidism is suspected. Ask for free T4 alongside TSH, and ask what the reference range for your result was; ranges vary between labs.
- Sleep disorder screening. If you have persistent unexplained fatigue, disrupted sleep, morning headaches, or low mood, ask your doctor about a referral for a sleep study. Tell them you do not snore. This matters for female presentation.
- Vitamin B12. Research estimates that vitamin B12 deficiency affects 10% to 15% of people over age 60, and absorption of food-bound B12 is lower in older adults, associated with reduced stomach acid production.¹² Fatigue, cognitive slowing, and mood changes are recognized symptoms. Ask for serum B12 if these are present.
- Depression screening using a validated tool. Ask your doctor to use a formal depression screening tool, not just a conversational check for sadness. The Geriatric Depression Scale specifically accounts for physical and somatic presentations in older adults.
Freely accessible information on each of these tests, including plain-language explanations of what they measure, is available at MedlinePlus (medlineplus.gov/lab-tests/). No account or membership is required.
None of these tests is exotic. None requires a specialist referral to order. Has your doctor been asked for all five?
Your Exhaustion Has a Name. Find It.
The exhaustion you have been told to accept is often the signature of something findable. Fatigue in women over 55 that persists despite adequate sleep is a signal, not a verdict.
Subclinical thyroid dysfunction, undiagnosed sleep apnea, low ferritin, and depression presenting as physical exhaustion each produce it, and each goes undetected by standard screening.
Ask your doctor to test your ferritin, TSH, B12, and a sleep disorder screening at your next visit, not because something must be wrong, but because something might be fixable. But this is not what aging has to feel like.
⚠️DISCLAIMER:
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The content addresses unexplained fatigue in women over 55 and its potential medical causes and is intended for general educational purposes only. Health conditions vary significantly between individuals, always consult a licensed physician or qualified healthcare provider before making any decisions about your health or medical care.
References
- Chiu HH, Tsao LI, Liu CY, Lu YY, Shih WM, Wang PH. The Perimenopausal Fatigue Self-Management Scale Is Suitable for Evaluating Perimenopausal Taiwanese Women’s Vulnerability to Fatigue Syndrome. 2021. PMCID: PMC8002518. https://pmc.ncbi.nlm.nih.gov/articles/PMC8002518/
- Taylor-Swanson L, et al. The Dynamics of Stress and Fatigue across Menopause: Attractors, Coupling and Resilience. Menopause. 2018. PMCID: PMC5866170. https://pmc.ncbi.nlm.nih.gov/articles/PMC5866170/
- Verdon F et al. Iron supplementation for unexplained fatigue in non-anaemic women: double blind randomised placebo controlled trial. BMJ. 2003. https://pubmed.ncbi.nlm.nih.gov/12763985/
- Morgan C, Ma A, Rivenbark J, Cotten S, Wilson S, Berkowitz C, Neutze D. Ferritin reference ranges and improving diagnosis of iron deficiency without anemia. Blood. 2025;146(Supplement 1):2609. doi:10.1182/blood-2025-2609. https://ashpublications.org/blood/article/146/Supplement%201/2609/550248/
- Mei Z, Addo OY, Jefferds MED, Brittenham GM. Physiologically based serum ferritin thresholds for iron deficiency in US older adolescents and adults. Blood Red Cells & Iron. 2026;2(1):100029. doi:10.1016/j.brci.2025.100029. https://ashpublications.org/bloodrci/article/2/1/100029/547478/
- Jain C, Mishra N, Singh S, Nirat A. Prevalence and risk factors of subclinical hypothyroidism in postmenopausal women: A cross-sectional study. Bioinformation. 2025;21(7):2241-2244. PMCID: PMC12569926.. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12569926/
- Floriani C et al. Effect of thyroid hormone therapy on fatigability in older adults with subclinical hypothyroidism: a nested study within a randomized placebo-controlled trial. Journal of Gerontology. 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7494024/
- Geer JH, Hilbert J. Gender Issues in Obstructive Sleep Apnea. Women’s Health (Lond). 2021. PMCID: PMC8461585. https://pmc.ncbi.nlm.nih.gov/articles/PMC8461585/
- Jehan S, Auguste E, Zizi F, Pandi-Perumal SR, Gupta R, Attarian H, Jean-Louis G, McFarlane SI. Obstructive Sleep Apnea: Women’s Perspective. J Sleep Med Disord. 2017;4(3). PMCID: PMC5323064.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5323064/ - National Institute of Mental Health. Older Adults and Mental Health. 2024. https://www.nimh.nih.gov/health/topics/older-adults-and-mental-health
- Harrison F, Mortby ME, Guastella AJ, Trollor JN, Mather KA, Sachdev PS, Brodaty H. Apathy and fatigue, but not depression, associated with inflammatory biomarkers in older adults. Int J Geriatr Psychiatry. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11710254/
- National Institutes of Health Office of Dietary Supplements. Vitamin B12: health professional fact sheet. NIH ODS. 2024. https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
- Martens K, DeLoughery TG. Sex, lies, and iron deficiency: a call to change ferritin reference ranges. Hematology Am Soc Hematol Educ Program. 2023;2023(1):617-621. doi:10.1182/hematology.2023000494. https://ashpublications.org/hematology/article/2023/1/617/506479/Sex-lies-and-iron-deficiency-a-call-to-change


