
Your doctor hands you a DEXA scan report. She says your bones look thin for your age. You drive home wondering if there’s anything you can actually do or whether bone loss is just something that happens now. Most people in that situation get the same advice: take calcium, go for walks, be careful not to fall. And that advice isn’t wrong, exactly.
But it’s incomplete. And for a lot of people, it isn’t working. Here’s what the research says: bone loss after 50 is real, but it is not a one way street. With the right type of exercise and the right nutrition, you can build bone density, not just slow the decline. Even after menopause. Even with osteopenia already diagnosed.
The evidence behind that claim provides you with a practical protocol to act on it. 54 million, Americans aged 50 and older have osteoporosis or low bone mass, putting roughly half of all adults in this age group at risk of a broken bone. Source: Bone Health & Osteoporosis Foundation.
Why Bone Density Drops After 50 — And Why That’s Not the End of the Story?
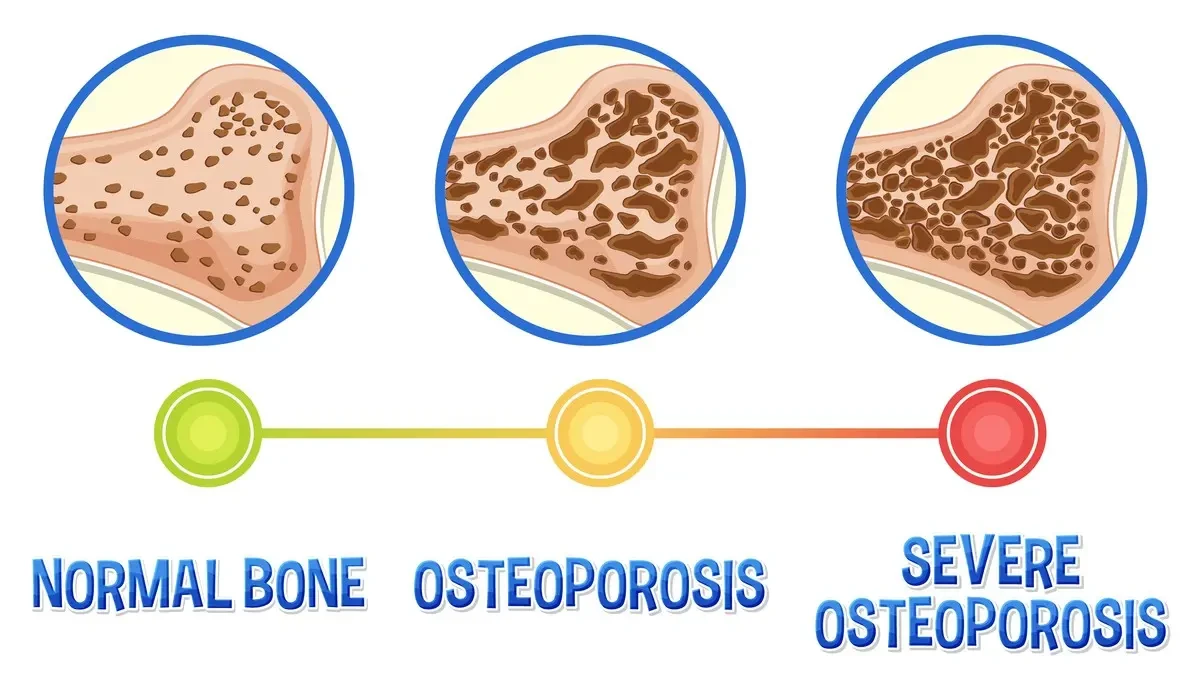
Your bones hit peak density somewhere in your late 20s. After that, they slowly start to thin. Around age 40, the process picks up speed. After menopause, it accelerates again. Your body uses two types of bone cells. Osteoblasts build new bone. Osteoclasts break old bone down. They work as a team. But when estrogen drops after menopause, the balance shifts.
The breakdown crew gets faster. The building crew slows down. Bone mass falls. This is how osteopenia happens. Osteopenia means your bones are thinner than normal but not yet at the level of osteoporosis. A T score between 1.0 and 2.5 puts you in that range. A score below 2.5 indicates osteoporosis. And roughly 48% of adults over 50 fall somewhere in the osteopenia zone.
Most people don’t know they’re in that zone at all. 69% of people with osteoporosis in the U.S. go undiagnosed. In the 50 59 age group, that figure rises to nearly 85%. Most people find out only after a fracture. The fracture risk is serious. One in two women over 50 will break a bone in their lifetime due to osteoporosis.
Hip fractures are the most dangerous; they come with significant recovery challenges and carry real risks in the year that follows. But here’s the part most people never hear: bone is living tissue. It responds to stress. When you put the right kind of load on a bone, it gets the signal to rebuild. This happens at any age. The question is what kind of load actually triggers that response.
The Science: How Strength Training Actually Builds Bone?
When a muscle contracts hard against resistance, it pulls on the bone it’s attached to. That pull creates mechanical tension inside the bone. And that tension sends a message to the osteoblasts: build more here. This process is called mechanotransduction. You don’t need to remember the word. Just remember the principle: muscle pulls bone, bone gets the signal, bone builds back.
The problem with walking, yoga, or gentle exercise is that they don’t create enough tension to trigger that process in a meaningful way. Your body adapts to low load movement quickly. The bone stops responding. You plateau. What bone responds to is high magnitude strain delivered at a high rate. In plain terms: lifting heavy things. And doing it progressively, so the load keeps increasing over time.

Key Study — LIFTMOR Trial (2018)
Australian researchers tested this directly. Postmenopausal women with low bone mass followed a twice weekly high intensity resistance and impact training program for 8 months. The results were significant. Compared with the low-intensity group, the heavy training group showed approximately 4% higher bone density at the lumbar spine and 2% higher at the femoral neck.
Only one minor adverse event occurred across the entire study. Average adherence was above 90%: Watson SL et al., Journal of Bone and Mineral Research, 2018. The LIFTMOR trial was a turning point. Before it, researchers were hesitant to prescribe heavy lifting to women with osteoporosis. They worried about fracture risk.
The trial showed those concerns, while understandable, were holding people back from the one thing that actually works. And the evidence has only grown since then.
2025 Meta-Analysis — 17 Studies, 690 Women
A 2025 systematic review published in the Journal of Orthopaedic Surgery and Research pooled results from 17 randomised controlled trials. The conclusion was clear: resistance training significantly improves bone density at the lumbar spine and femoral neck in postmenopausal women. Programs working at greater than 70% of maximum capacity showed the strongest results.
Journal of Orthopaedic Surgery and Research, May 2025, PMC 12107943. How much improvement is realistic? Long term programs of 4 to 6 months using moderate to heavy loads, 2 to 3 sessions per week, have shown bone density increases of up to 3.8% at the spine and hip. Doctors consider that clinically meaningful. It’s not a small number.
The Bone-Strengthening Protocol: The Big Four Movements
The goal of every exercise in this protocol is the same. You want to create enough tension in a muscle that it pulls hard on the bone. That pull triggers the bone to rebuild. And that requires load. Real load.
Here is the framework that research supports.
| Variable | Target | Notes |
|---|---|---|
| Frequency | 2–3 sessions/week | At least one full rest day between sessions. This matches both the LIFTMOR protocol and the 2025 meta-analysis consensus. |
| Intensity | 8–12 reps to fatigue | The last 2–3 reps should be genuinely hard with good form. Working at 70 85%+ of your maximum produces the best bone results. |
| Sets | 3–5 per exercise | The LIFTMOR protocol used 5 sets of 5 reps at above 85% of maximum. For beginners, start with 3 sets of 8–12. |
| Progression | Add load regularly | Add 1–2 kg when all reps feel manageable. If you don’t progress the load, the bone stops adapting. This is non-negotiable. |
| Impact sessions | 1–2 extra sessions/week | Jumping, jogging, skipping rope, or marching in place. Ground reaction forces add compression signals that complement the strength work. |
The Big Four Movements
These four movement patterns cover the major muscle groups. Together, they load the bones most at risk from osteoporosis the hip, spine, femoral neck, and wrist.
1. Squat

Targets: Hip · Lumbar spine. This loads the hips and lower spine directly, two of the most common fracture sites. Start with a goblet squat, holding a dumbbell or kettlebell at your chest. Beginner: bodyweight or goblet squat. Intermediate: barbell back squat or leg press.
2. Hinge (Deadlift)

Targets: Femoral neck · Lower spine. The femoral neck is one of the most fracture prone spots in the body. Hinging movements load it directly. A Romanian deadlift with dumbbells is a safe starting point. Beginner: hip bridge or Romanian deadlift. Intermediate: trap bar or barbell deadlift.
3. Pull (Row)

Targets: Upper spine · Shoulder girdle. The upper back and vertebrae are common sites for vertebral fractures. Pulling movements load the muscles that pull on those bones and help reverse the rounding that comes with bone loss. Beginner: seated cable row or resistance band row. Intermediate: lat pulldown or dumbbell row.
4. Push (Press)

Targets: Wrist · Shoulder · Thoracic spine. Wrist fractures from falling are one of the earliest signs of bone weakness. Pressing movements build the strength and bone density in the arm and shoulder to protect against them. Beginner: wall push up or seated dumbbell press. Intermediate: overhead barbell press or floor press.
Nutrition: Your Bones Need More Than Just Calcium
Think of training as the construction crew and nutrition as the building materials. You can have the best crew in the world. But if you don’t give them what they need to build, nothing gets made. Four nutrients matter most for bone health after 50.
Calcium

Women 51+: 1,200 mg/day | Men 51 70: 1,000 mg/day. Calcium is the main mineral in bone. Get it from food first dairy, leafy greens (kale, bok choy), canned sardines or salmon with bones, and fortified plant milks. Supplements fill the gap if food isn’t enough, but they’re not a substitute.
Vitamin D

Adults 50+: 800–1,000 IU/day. Without enough Vitamin D, your body can’t absorb calcium properly. Even good calcium intake won’t reach the bone if Vitamin D is low. Sun exposure helps, but most people over 50 need a supplement to reach optimal levels. Get your blood level tested.
Protein

0.8–1.6 g per kg of body weight/day. Bone is about 50% protein by weight. Most people don’t think of protein as a bone nutrient, but it’s essential. Higher protein intake is linked to higher bone density. Active older adults likely need the upper end of the range. Think eggs, lean meat, fish, legumes, and Greek yoghurt.
Vitamin K2 & Magnesium

Supporting nutrients get from food, Vitamin K2 helps direct calcium into bone instead of blood vessels. Magnesium activates Vitamin D and is part of the bone matrix. Good sources: fermented foods, K2, dark leafy greens, nuts, seeds, and legumes, and magnesium.
How to Get Started: A Practical 12-Week Entry Plan
The biggest barrier most people face isn’t motivation. It’s not knowing where to start without hurting themselves. Here’s a phased plan that takes you from zero to a full bone building protocol over three months. But first, one thing before you begin. If you haven’t had a DEXA scan in the last two years, get one.
Ask your GP or gynaecologist for a referral. Know your T score before you pick up a barbell. If it’s below 2.0, work with a specialist first. The plan below is designed for people at the osteopenia level or those starting as a preventive measure.
Weeks 1–4: Learn the movements — build the foundation
- 2 sessions per week. Focus entirely on form, not weight.
- Squat: bodyweight or goblet squat with a light dumbbell. Hinge: hip bridge on the floor.
- Pull: seated band row or cable row with very light resistance. Push: wall push ups or seated dumbbell press with 24 kg.
- Add 10 minutes of brisk walking or marching after each session.
- Goal: feel confident in each movement, no joint pain, no dizziness.
Weeks 5–8: Add load — make the last reps genuinely hard
- 2 3 sessions per week. Add resistance bands, dumbbells, or cable machines.
- Aim for 1012 reps per set. The last 2 3 should feel challenging, not painful, but genuinely hard.
- Add one impact session per week: 10 minutes of step ups, stair climbing, or light jogging.
- Keep a simple training log. Write down the weight, sets, and reps each session.
Weeks 9–12: Progressive overload — this is where the bone adapts
- 3 sessions per week of strength training. 2 impact sessions per week.
- When all reps feel manageable, increase the load by 510%. Then drop to 8 to 10 reps per set.
- Focus on the Big Four: squat, hinge, pull, push every session.
- Re assess DEXA at 6 and 12 months from your baseline scan. BMD changes are slow. Do not judge progress by how you feel, but by how you measure it.
Conclusion
Bone loss after 50 is real. But it is not something you just have to accept. Progressive resistance training, such as squats, deadlifts, rows, and presses, is the most evidence backed way to build bone density after 50. The LIFTMOR trial proved that this works even in women with osteopenia and osteoporosis, safely, with proper guidance
Calcium, Vitamin D, and protein are the raw materials your body needs to actually rebuild after you train. Cutting back on smoking and heavy alcohol use removes two major obstacles to bone recovery. A consistent program of 4 6 months is where real, measurable change happens, not a 2 week experiment.
⚠️MEDICAL DISCLAIMER
This article is for informational purposes only. It does not replace medical advice, diagnosis, or treatment. Before changing your exercise routine, diet, or supplement use, talk to your doctor first. If you experience chest pain, dizziness, severe joint pain, or any sudden symptom during exercise, stop and seek medical care immediately.


