You were told it would fix the burning. It did. So you kept taking it, morning after morning, year after year, the way you take any tool that works. No one mentioned that the thing your body uses to burn had forty other jobs.
For adults over 50 taking a daily heartburn pill, the prescription often keeps renewing because the discomfort returns when they stop, but most people don’t know that the return of symptoms can itself be caused by the drug.
Long-term PPI risks are the problem this article addresses: what acid suppression actually removes from the rest of your body while it quiets your chest.
Why reading this is worth your time:
- The reason stopping the pill makes heartburn worse than before you started it
- What your bones, nerves, and gut bacteria all have to do with your heartburn prescription
- The specific question your doctor may never have asked about whether you still need this medication
- Why some of the risks accumulate slowly enough that neither you nor your doctor noticed
- What the evidence shows about getting off these drugs safely
What stomach acid actually does inside your body every day
You probably think of stomach acid as the villain. That’s exactly what the drug was designed to make you think. Acid is not a flaw in the system. It is the system, doing several jobs at once.
Protein digestion starts here. When you eat a chicken breast or a handful of almonds, your stomach secretes hydrochloric acid to break protein apart so digestive enzymes can finish the job.¹
Without an acidic environment, the enzyme pepsinogen [the inactive precursor that converts into pepsin, the main protein-digesting enzyme] cannot activate, and protein arrives in your small intestine only partially broken down.¹
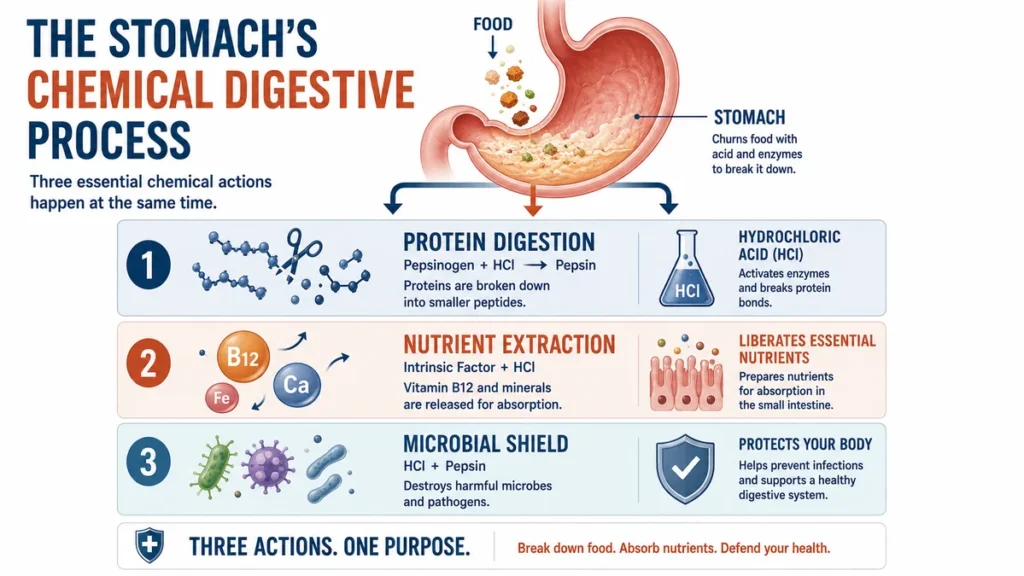
Nutrient release depends on it. Stomach acid frees vitamin B12 from the proteins it travels bound to in food.² It also releases iron and calcium so the intestine can absorb them.² These are not minor functions. B12 supports nerve signaling. Iron carries oxygen in the blood. Calcium keeps bone dense.
Bacteria don’t like it. Every piece of food you eat carries microbes.¹ The stomach’s low pH kills or slows most of them before they reach the intestine.¹ When you significantly raise the pH, you remove that filter.
You have been taking a drug that suppresses all three of those functions simultaneously. That is not a criticism of the drug when used correctly. It is a description of what the drug does, which should be on the label.
Long-term PPI risks reach well beyond heartburn.
The rebound trap: why stopping feels harder than starting
Your body adapted to the drug. When you stop taking it, the adaptation doesn’t disappear overnight. What you feel when you quit is not always your original condition coming back.
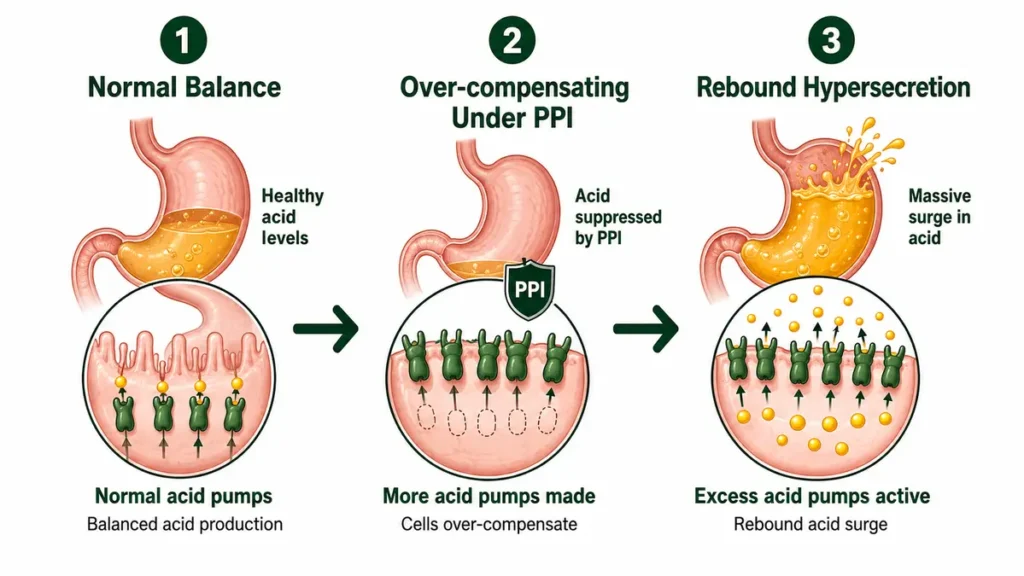
Rebound acid hypersecretion [a spike in stomach acid output that occurs after stopping an acid-suppressing drug, often exceeding pre-treatment levels] is what happens when prolonged acid suppression ends.³
The stomach, which had been compensating for suppressed output by increasing certain signaling activity, releases that compensation all at once.³ The result can be acid output higher than it was before treatment began.
Research has directly tested this. Healthy volunteers with no prior history of heartburn or reflux were given a PPI for eight weeks, then taken off it.⁴,³
About 40 to 50 percent developed new reflux or heartburn symptoms after stopping, symptoms they had never experienced before the study.⁴,³ The control group, which received placebo, had no such symptoms.
That finding has a name: a drug that produces the condition it was prescribed to treat.
Daily PPI exposure for more than four weeks is likely to trigger rebound acid hypersecretion within about 15 days of stopping, with symptoms lasting days to several weeks depending on how long the drug was used.⁴ The longer the exposure, the stronger the rebound signal.
This is why people stay on these drugs longer than intended. The symptom return feels like proof they still need the medication. In many cases, it is proof the medication changed their physiology, and the change needs time to reverse.
No single study tests the full chain of long-term PPI effects. The picture assembled here draws on separate research bodies, each testing a different outcome in a different population.
What long-term acid suppression removes from the body
You have likely never seen a list of what your heartburn drug removes. Almost none of them focus on what the drug takes away.
The pill fixed the symptom by dismantling the system that was creating it, and what that system does for the rest of your body is not on the label.

Vitamin B12 depletion. A systematic review of older adults taking PPIs for six months or more found a 12 to 18 percent reduction in serum vitamin B12 over 12 months of use.⁵
B12 is not stored in large amounts in the body. When levels fall, nerves are among the first structures to feel it.
Calcium and bone turnover. In the same review population, calcium and parathyroid hormone [the signaling hormone that directs calcium in and out of bone] levels declined, while markers of bone breakdown increased despite stable bone mineral density.⁵ The structural cost was accumulating before it could be measured by a standard bone scan.
Magnesium reduction. Evidence on magnesium is less consistent, but some populations showed changes in how the mineral was handled by the body, even when blood levels appeared normal.⁵
People on PPIs for more than one year showed 11.6 times higher odds of vitamin B12 deficiency and 12.8 times higher odds of magnesium deficiency compared to non-users, in a retrospective study of 312 adult patients.⁶
These are not rare outcomes. They are documented, measurable, and largely invisible until something breaks.
How these risks land differently when you are over 50
The nutrient depletions described above affect everyone who takes these drugs long-term. After 50, the margin is thinner.
Bone mass naturally declines with age. Gut absorption naturally slows. B12 absorption from food already depends on a stomach enzyme that becomes less reliable as people age.⁷
When a daily drug further reduces acid output for years, these age-related changes and drug-related changes compound each other. A systematic review found that PPI-related nutrient losses may contribute to cognitive decline, bone fragility, and increased fall risk specifically in elderly and comorbid populations.⁷
Fracture risk is the best-documented outcome. A multicenter cohort study found that PPI use was associated with a shorter time to first fracture in adults 25 and older, after adjusting for bone density and other risk factors, with a hazard ratio of 1.40.⁸
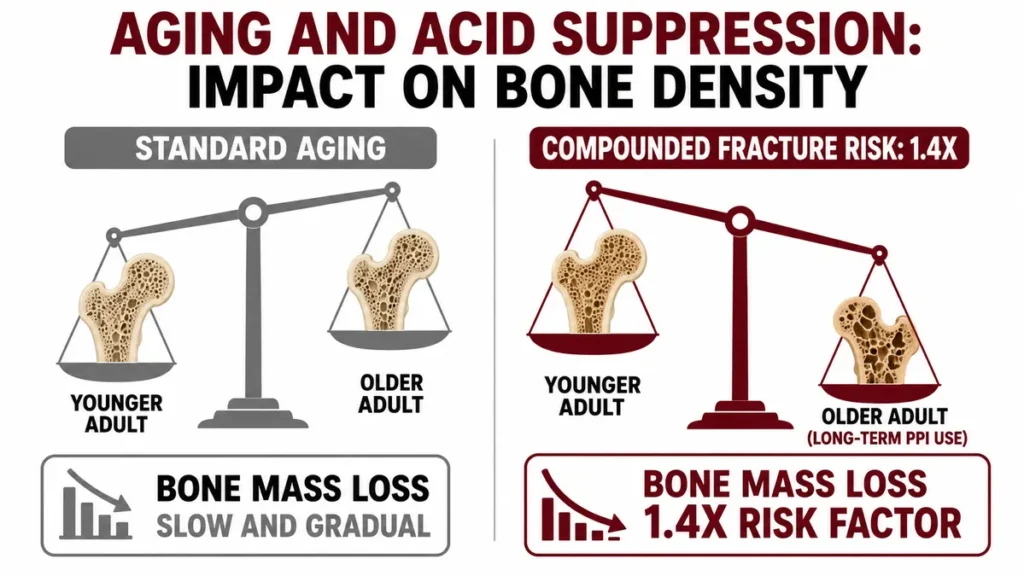
A separate analysis of women aged 60 to 79 with prior fracture risk factors found a hazard ratio of 1.2 for PPI users versus non-users.⁸
This is where the evidence needs an honest qualifier. Observational studies dominate this field. That means the associations are real and consistent, but causation has not been proven by a controlled trial for most of these outcomes.⁷
People with serious illness are more likely to take PPIs long-term, and serious illness independently raises fracture, kidney, and cognitive risk. The studies attempt to control for this. They do not eliminate the possibility.
What the evidence does show, clearly and across multiple independent datasets, is that the pattern of association is too consistent to ignore, and that older adults face it with less reserve.
Aging means the same drug is a different exposure.
What your doctor can check before the next refill
Most people who are on a PPI today started it for a reason that may no longer apply. The refill is not a re-evaluation. It is a default.
Guidelines from the American Gastroenterological Association recommend that patients should not continue any medication when there is no reasonable expectation of benefit based on evidence or prior treatment response.⁹
A reasonable check-in with your doctor before the next refill, especially if you have been on a PPI for more than a year, could include reviewing the items below.

Talk with your doctor before changing or stopping any prescribed medication, and especially before stopping a PPI abruptly if you have been on one long-term, since rebound symptoms can be significant.
Before your next refill, ask about:
- Whether a documented diagnosis still requires this drug, or whether it was started for a short-term reason and carried forward
- Serum vitamin B12 levels, since low B12 from PPI use can develop before symptoms appear
- Serum magnesium, particularly if you take the drug daily and have been doing so for more than six months
- Bone density (DEXA scan) if you have been on a PPI for more than two years and have additional fracture risk factors such as low body weight, prior fracture, or family history of osteoporosis
- Whether a dose reduction or on-demand use (taking the drug only when symptoms occur) could replace daily use
- Whether a short course of an H2 blocker could manage your symptoms during a step-down from a PPI
Evidence supports dose reduction and on-demand use as reasonable deprescribing strategies, particularly for people with non-erosive reflux disease or no complicated GI history. Some clinical guidance also suggests H2 receptor antagonists [an older class of acid-reducing drugs, such as famotidine, that work through a different receptor than PPIs] may be used as part of a step-down approach.¹⁰
One question that could change your next prescription
The most common reason people stay on a PPI indefinitely is that no one reviewed whether the original reason still exists. The prescription renews because no one stops it.
Research shows that an estimated 25 to 70 percent of PPI users may not have an appropriate current indication for the drug, depending on the clinical setting.¹¹
A meta-analysis of 79 studies covering more than 20,000 patients found a pooled rate of inappropriate PPI overuse of 60 percent.¹¹ That is not a small edge case.
Deprescribing, defined as the supervised reduction or stopping of a medication no longer needed, is considered safe for most patients taking PPIs for GERD or mild esophagitis.¹⁰ It does not require abrupt stopping.

Strategies include cutting the dose by half at one-to-two-week intervals, moving to every-other-day dosing, or shifting to on-demand use, where the drug is taken only when symptoms appear rather than every morning.¹²
None of this requires diagnosing yourself or deciding alone. A practical resource is available at deprescribing.org, where the Canadian Deprescribing Network publishes free, clinician-developed patient decision aids for reviewing PPI use with your doctor.
The drug works. The question is whether it still needs to be doing that job every single day, in your body, at your age.
The renewal isn’t the original problem
The pill wasn’t wrong. What was wrong was the assumption that taking it indefinitely was free. The long-term PPI risks documented here are nutrient depletion, bone metabolism shifts, and gut defense reduction, all compounding against a body already managing the changes of aging after 50.
Ask your doctor this question at your next visit: “Do I still have a documented reason to take this, or has it just carried over?” Many people find the answer is no. Whether yours is yes or no is a question this article cannot answer for you.
⚠️DISCLAIMER
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The content addresses the risks of long-term proton pump inhibitor use and is intended for general educational purposes only. Health conditions vary significantly between individuals, always consult a licensed physician or qualified healthcare provider before making any decisions about your health or medical care.
References
- Hsu M, Safadi AO, Lui F. Physiology, Stomach. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2023 Jul 17. https://www.ncbi.nlm.nih.gov/books/NBK535425/
- Schubert ML. Gastric secretion. Curr Opin Gastroenterol. 2014 Nov;30(6):578-82. doi:10.1097/MOG.0000000000000125. PMID: 25211241. https://pubmed.ncbi.nlm.nih.gov/25211241/
- Namikawa K, Björnsson ES. Rebound Acid Hypersecretion after Withdrawal of Long-Term Proton Pump Inhibitor (PPI) Treatment—Are PPIs Addictive? PMC. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11122117/
- Rochoy M, Dubois S, Glantenet R, Gautier S, Lambert M. Gastric acid rebound after a proton pump inhibitor: Narrative review of literature. Therapie. 2017. https://pubmed.ncbi.nlm.nih.gov/29195714/
- Shahid MS, Ahmed N, Kamal Z, Nathaniel L, Singla B, Singla S, Kumawat S, Batool M, Ekomwereren O, Anika NN, Sahil M. A Systematic Review of Long-Term Use of Proton Pump Inhibitors (PPIs) in Older Adults on Polypharmacy: Do PPIs Deplete Nutrients? PMC. 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12456669/
- Kotkata F, Koraiem K, Altaras R, Zaki M, Abdelwahab D, Elias M, Abo Alhassan M, Elsaidy M, Elmeligy E, Awad E, Youssef B, Ahmed A, Khalafallah N, Mousa A, Elsafty W, Elkady A. Association Between Long-Term Proton Pump Inhibitor Use and Deficiency of Vitamin B12 and Magnesium in Gharbia, Egypt: a Retrospective Study. J Basic App Pharmacol. 2025;5:O94-103. https://li01.tci-thaijo.org/index.php/JBAP/article/view/269139
- Chaudhry M, Elahi M, Bukhari SHA, Ibikunle D, Koirala A, Ahmed SZ, Mastoi MG, Jabeen N, Lal K, Khan A, Ali U. Long-Term Proton Pump Inhibitor Use and the Risk of Kidney Disease, Dementia, and Fractures: A Systematic Review. PMC. 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449571/
- Paudel Y, Najam B, Desai HN, Illango J, Seffah KD, Kumar M, Naveen N, Pachchipulusu VK, Penumetcha SS. Use of Proton Pump Inhibitors and Risk of Fracture in Adults: A Review of Literature. PMC. 2023. PMCID https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10760937/
- Targownik LE, et al. AGA Clinical Practice Update on De-Prescribing of Proton Pump Inhibitors: Expert Review. Gastroenterology. 2022. https://www.gastrojournal.org/article/S0016-5085(21)04083-X/fulltext
- Rossi A, Perrella L, Scotti S, Olmastroni E, Galimberti F, Ardoino I, Orlando V, Menditto E, Franchi C, Casula M. Approaches to Deprescribing Proton Pump Inhibitors in Clinical Practice: A Systematic Review. Pharmaceuticals. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11508458/
- Jearth V, Dutta A, Sharma V. Misuse of Proton Pump Inhibitors: Time for PPI Stewardship. World Gastroenterology Organisation e-WGN. 2024 Sep;29(3).https://www.worldgastroenterology.org/publications/e-wgn/e-wgn-expert-point-of-view-articles-collection/misuse-of-proton-pump-inhibitors-time-for-ppi-stewardship
- Therapeutics Initiative, University of British Columbia. Deprescribing Proton Pump Inhibitors. Therapeutics Letter. 2018 Apr;(111). https://www.ncbi.nlm.nih.gov/books/NBK598442/