
You have tracked your meals, cut the carbs, skipped the wine, and still watched the scale sit there like it is enjoying the standoff. Adults who eat well and still cannot lose weight are not failing at willpower.
They are failing at a problem that diet alone was never designed to solve. This article explains why diet alone rarely solves a weight problem when your hormones, sleep, stress response, and daily movement patterns are working against you.
The real question is not what you are eating. It is why your body refuses to let it go.
Why reading this will change what you do next:
- Discover why one night of poor sleep shifts your hunger hormones before breakfast even arrives
- Find out why the movement between your workouts burns more calories than the workouts themselves
- Learn what chronic stress deposits in your midsection that no food swap can touch
- Understand why your thyroid might be silently slowing your metabolism without showing on a routine blood panel
- See the four lab tests to request before changing your diet again
Why Your Hunger Hormones Betray You After One Bad Night of Sleep
You eat clean all week and then, after one rough night, you find yourself standing at the pantry at 10 am reaching for something you would never normally touch. That is not a character flaw.
That is a hormone shift, and it happens fast enough to derail why you cannot lose weight before your first meal of the day.
Sleep and hunger are linked through two hormones most people have never heard of. Leptin [the hormone that signals fullness and tells your brain to stop eating] drops when you sleep poorly. Ghrelin [the hormone that drives hunger and pushes you toward calorie-dense food] rises in response.
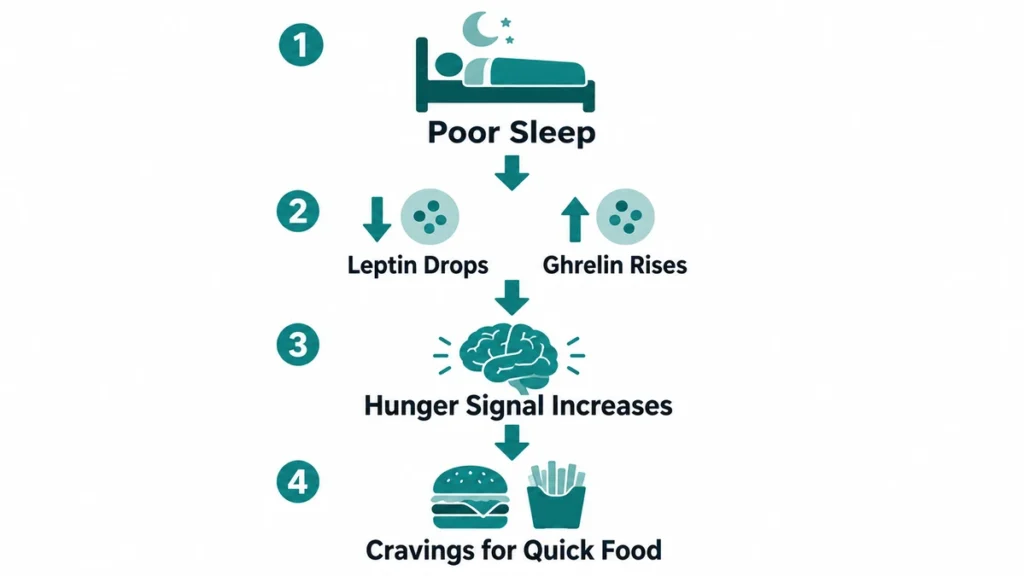
A 2023 laboratory study published in Obesity measured both hormones in 44 adults after one night of total sleep deprivation compared to a full night of sleep.¹
After the sleepless night, fasting leptin levels fell while ghrelin levels rose, changes the researchers noted could facilitate weight gain if sleep loss persisted over time.¹
You have lived through this. You know what a tired Tuesday does to your food choices. What the research adds is a biological reason why willpower feels so thin when you are running low on sleep, your hormones are already working against you before you open the refrigerator.
Sleep debt is not a mood problem. It is a hormonal one.
The gap between what you eat and what your body does with it begins the night before, not at the table. That is all it takes to shift the biology working underneath your choices.
Why the Activity Between Your Workouts Matters More Than the Workouts Themselves
Most people who struggle with weight loss and NEAT think they are solving the problem by going to the gym three times a week. The hour on the treadmill matters. What happens the rest of the day matters more.
Non-exercise activity thermogenesis, or NEAT [the total energy your body burns through every movement that is not formal exercise: walking to your car, shifting in your chair, carrying groceries, standing at a counter] is the most overlooked variable in weight management.
Research published in Journal of Internal Medicine found that NEAT could account for up to 2,000 calories of difference in daily energy expenditure between two people of similar body size.²
The calories you burn walking to the kitchen, fidgeting in your chair, and standing at your counter can vary by up to 2,000 per day between two people eating identical meals, which means the gap in your weight loss may have nothing to do with your fork.²
That number is not a rounding error. A 2022 review published in Frontiers in Public Health documented a decades-long shift toward desk-based work and noted that this decline in low-intensity daily movement is a significant factor in rising obesity rates, independent of whether people exercise deliberately.³
Daily movement patterns shape calorie output in ways that structured workouts simply cannot compensate for. Someone who sits for nine hours at a desk and then completes a 45-minute run burns fewer total calories than someone who never runs but stays on their feet most of the day.
What does your day look like between the workouts you are already doing?
What Chronic Stress Does to Belly Fat That No Salad Can Undo
Beyond what you move, there is what you carry. Stress does not just make you reach for the chips. It tells your body exactly where to store fat, and it picks the one location that is hardest to shift.
Cortisol [a stress hormone released by the adrenal glands when the body perceives a threat, whether real or psychological] is the mechanism most weight-focused conversations skip entirely.
A 2025 comprehensive review published in Clinical Obesity found that chronic exposure to elevated cortisol is increasingly linked to obesity, with the stress-response system playing a central role in how persistent pressure disrupts fat distribution.⁴
Abdominal fat tissue has a higher concentration of cortisol receptors than fat stored elsewhere on the body. This means cortisol binds preferentially to belly fat cells, signaling them to expand and resist release.⁴
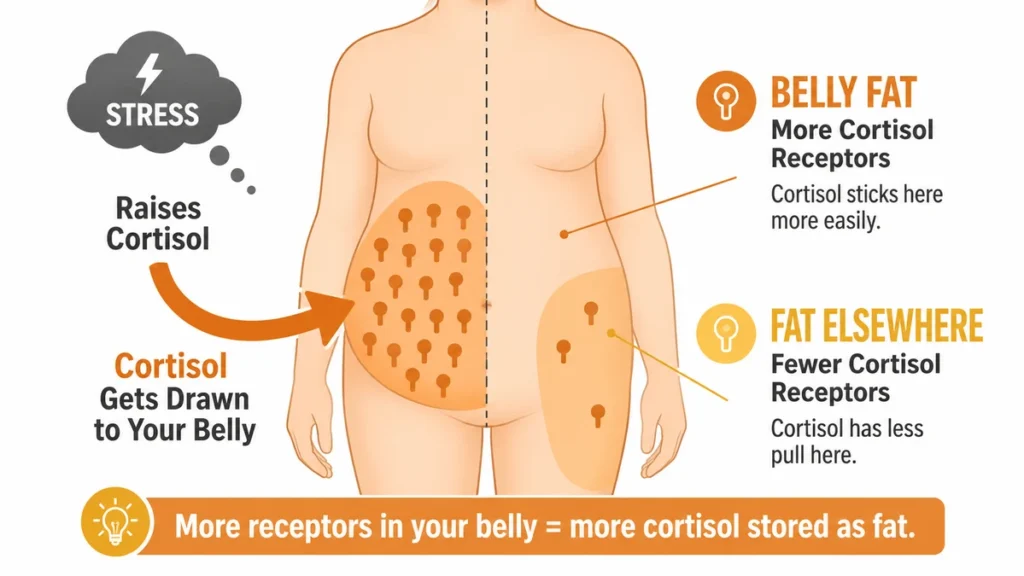
Stop blaming the appetite. The fat is accumulating in that location because the stress response is depositing it there. Cortisol is doing exactly what it evolved to do.⁴
That is the real finding here: storing energy in the most accessible location during a perceived emergency is not a malfunction. It is a feature running on the wrong timeline, and no food swap turns off the signal directing it.⁴
The direct challenge is this: if you cannot lose weight and cortisol is linked to abdominal fat accumulation in ways no diet addresses, then no amount of salad substitution touches the actual mechanism.⁴
Reducing calorie density does not turn off the signal telling your body where to put the fat it is holding onto.⁴
Chronic stress and weight interact at a level that food choice cannot reach. This is the piece most weight-loss advice never addresses, and it is the reason clean eating alone can feel like it accomplishes nothing visible.⁴
Stress is not a personality trait that some people have and others do not. It is a biological state that changes how your body uses every calorie you eat.
How Insulin Resistance Turns What You Eat Into Fat You Cannot Shed
You may have noticed that none of the causes named so far have anything to do with what is on your plate. That is the point.
The evidence making it comes from several different research areas, not one unified study. No single trial directly proves the complete argument this article is building.
Sleep research, cortisol research, metabolic research, and movement research each contribute one thread, and this article weaves them together. That is the honest account of what the science actually shows.
With that said, insulin resistance [a condition where the body’s cells stop responding properly to insulin, leaving excess glucose circulating in the blood rather than entering cells for energy] is one of the clearest examples of how a non-dietary mechanism can stall weight loss entirely.
A 2024 state-of-the-art narrative review published in the International Journal of Molecular Sciences concluded that individual variability in weight outcomes is significantly shaped by hormonal factors.⁵
Insulin sensitivity [how well the body’s cells respond to insulin’s signal to take up blood sugar] is among those factors, and the review positioned it as a reason calorie intake alone does not determine weight outcomes.⁵
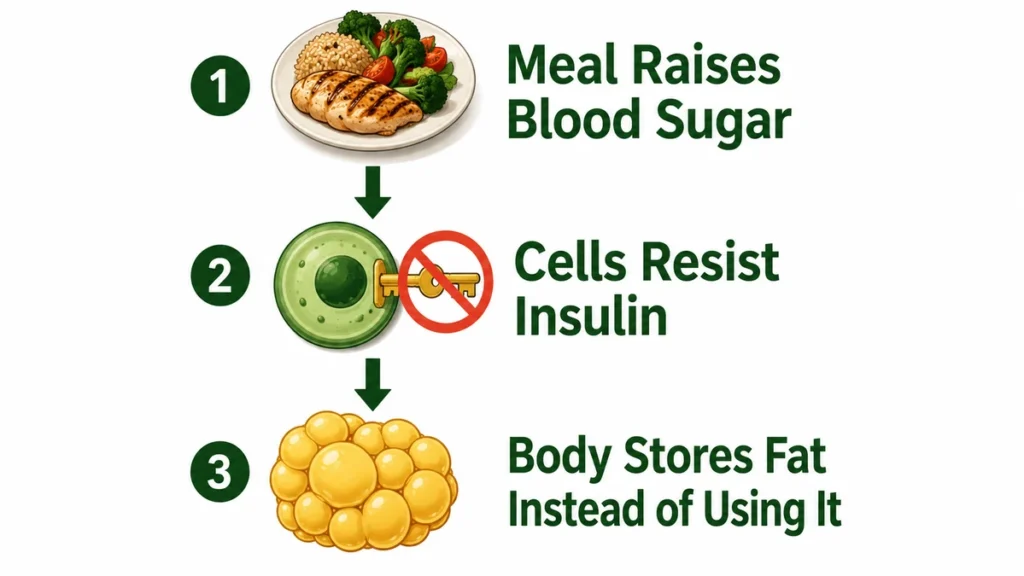
When cells resist insulin, the pancreas compensates by releasing more of it. Higher circulating insulin is associated with a shift toward fat storage rather than fat use.⁵
This is not about eating too much sugar. It is about a signaling failure that appears to push the body toward storing rather than using energy from ordinary meals.
A person eating a chicken breast and vegetables can still be accumulating fat if their cells are ignoring the insulin telling them to take up glucose.
Insulin resistance and weight loss do not coexist easily. A diet change may reduce glucose intake, but it does not restore the cell’s sensitivity to insulin on its own. The same review shows that movement, sleep, and stress reduction each also improve insulin sensitivity through distinct biological pathways—effects that simply cutting carbohydrates cannot replicate.⁵
If you have been eating less for months and watching the scale ignore you, insulin resistance is worth asking your doctor about.
How Your Thyroid Can Quietly Slow Your Metabolism Without Triggering a Diagnosis
You can eat carefully, exercise regularly, and still feel like your metabolism has stalled completely. In some cases, the gland responsible for setting your metabolic rate is running slow, but not slow enough to show up on a basic blood panel.
Subclinical hypothyroidism [a condition in which thyroid-stimulating hormone levels are mildly elevated but the main thyroid hormone, T4, stays within the normal range] is more common than most people realize.⁶

According to the NIH, its incidence in the general population ranges from approximately 3% to 15% depending on the group studied.⁶
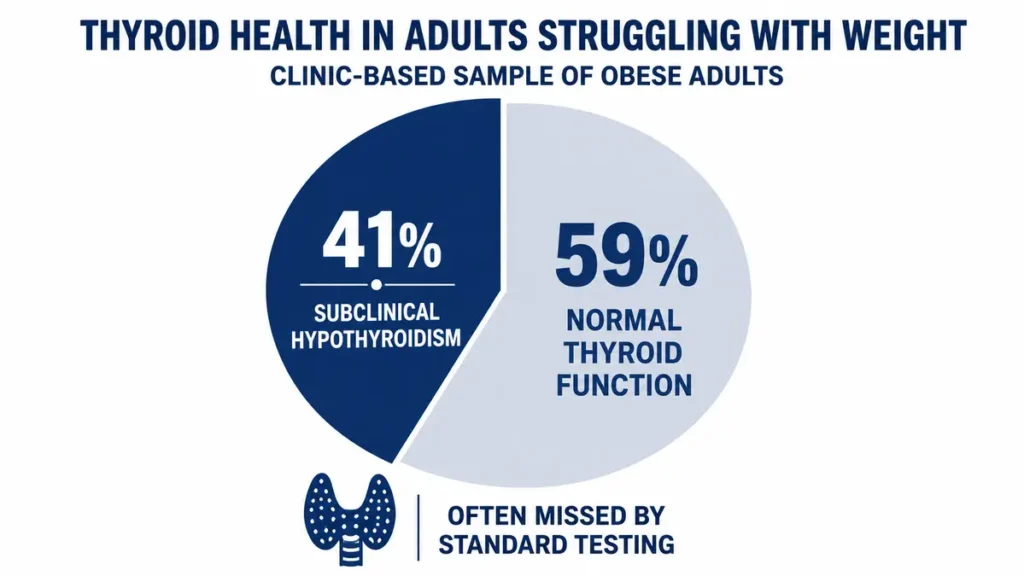
A 2025 prospective cohort study published in Cureus found that 41% of obese adults examined at an endocrinology clinic had subclinical hypothyroidism. Those patients had significantly higher measures of insulin resistance and worse metabolic markers compared to obese patients with normal thyroid function.⁷
That is a large proportion of people in a weight-affected population carrying a thyroid condition mild enough to be missed on routine testing.
The word “subclinical” does real harm here. It sounds minor. What it actually means is that the body’s thermostat has a problem that has not yet crossed an arbitrary diagnostic line.
Reduced thyroid hormone activity slows the body’s metabolic rate. This means the body simply burns fewer calories at rest and that happens independent of what a person eats or how often they exercise.⁶
Routine thyroid testing often stops at TSH alone. Free T3, free T4, and thyroid antibodies give a more complete picture of whether thyroid function is affecting your metabolic rate.
If you are trying to lose weight and your thyroid is running below its optimal rate, better food choices will not close that gap.
What to Tell Your Doctor Instead of Asking for Another Diet Plan
Most weight conversations with a doctor end at the same place: eat less, move more. If you have already done both and made no progress, that conversation needs different questions driving it.
The biology this article has covered (sleep-disrupted hunger hormones, cortisol-directed fat storage, insulin resistance, and slowed thyroid metabolism) is all measurable. These are not theories. They are biological states that show up in blood work and can be tested, identified, and addressed with support from a healthcare provider.

Talk to your doctor before changing any medications or starting a new treatment plan, especially if you are managing a chronic condition, are pregnant, or take prescription drugs that affect hormones or metabolism.
The four tests worth requesting:
- Fasting insulin and glucose: to screen for insulin resistance before it reaches a diabetes diagnosis
- Full thyroid panel (TSH, Free T3, Free T4, thyroid antibodies): to catch subclinical thyroid issues a TSH-only test misses
- Cortisol: a morning serum cortisol or 24-hour urinary cortisol can indicate whether the stress response is chronically elevated
- Sleep quality assessment: ask whether a sleep study or questionnaire-based screening is appropriate, since poor sleep architecture affects every other system in this article

The NIH National Heart, Lung, and Blood Institute offers a free public resource on overweight and obesity that covers metabolic testing and medical evaluation: https://www.nhlbi.nih.gov/health/overweight-and-obesity
Changing your diet is not wrong. But if you walk into your next appointment armed with the right questions, you give the conversation a chance to reach the variables that diet was never going to touch.
The Problem Was Never Your Plate
If you cannot lose weight despite eating well, you were not failing at dieting. You were solving the wrong problem.
Sleep, stress hormones, insulin resistance, and thyroid function each shape what your body does with the food you eat, and none of them appear on a nutrition label. Ask your doctor to check your cortisol, thyroid, fasting insulin, and sleep quality before changing your diet again.
What these tests reveal will depend entirely on your individual biology. That is the part no general advice can reach.
⚠️DISCLAIMER
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The content addresses why weight loss resistance occurs beyond diet and exercise and is intended for general educational purposes only. Health conditions vary significantly between individuals, always consult a licensed physician or qualified healthcare provider before making any decisions about your health or medical care.
References
- Egmond LT, Meth EMS, Engström J, Ilemosoglou M, Keller JA, Vogel H, Benedict C. Effects of acute sleep loss on leptin, ghrelin, and adiponectin in adults with healthy weight and obesity: A laboratory study. Obesity. 2023;31(3):635-641. https://pubmed.ncbi.nlm.nih.gov/36404495/
- Levine JA. Nonexercise activity thermogenesis – liberating the life-force. Journal of Internal Medicine. 2007.. https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2796.2007.01842.x
- Rizzato A, Paoli A, Bianco A, Palma A. Non-exercise activity thermogenesis (NEAT) and its role in the physiology of physical activity. Frontiers in Public Health. 2022;10:951995. https://pmc.ncbi.nlm.nih.gov/articles/PMC9650196/
- Lengton R, Schoenmakers M, Penninx BWJH, Boon MR, van Rossum EFC. Glucocorticoids and HPA axis regulation in the stress–obesity connection: A comprehensive overview of biological, physiological and behavioural dimensions. Clinical Obesity. 2025;15(2):e12725. doi:10.1111/cob.12725 https://pmc.ncbi.nlm.nih.gov/articles/PMC11907100/
- Theodorakis N, Kreouzi M, Pappas A, Nikolaou M. Beyond Calories: Individual Metabolic and Hormonal Adaptations Driving Variability in Weight Management—A State-of-the-Art Narrative Review. International Journal of Molecular Sciences. 2024;25(24):13438. PMCID: PMC11676201. PMID: 39769203. https://pmc.ncbi.nlm.nih.gov/articles/PMC11676201/
- Gosi SKY, Kaur J, Garla VV. Subclinical Hypothyroidism. In: StatPearls. StatPearls Publishing; 2024. Last Update: February 15, 2024 https://www.ncbi.nlm.nih.gov/books/NBK536970/
- Jameel U, Durrani O, Munib A, Khan A. Incidence of Subclinical Hypothyroidism in Obese Adults and Its Metabolic Implications: A Prospective Cohort Study. Cureus. 2025;17(4):e82248. doi:10.7759/cureus.82248. PMCID: PMC12661914. PMID: 41322799. https://pmc.ncbi.nlm.nih.gov/articles/PMC12661914/


