If you’re taking 5 mg of melatonin every night after 50 and still waking up at 2 AM, your dose isn’t the problem; your body is trying to tell you something else entirely. You’ve probably tried taking more. Still waking up. Still groggy in the morning.
Still wondering if something is seriously wrong. You’re not alone, and you’re not failing. Your body just processes melatonin completely differently now. Here’s what’s actually going on, and what sleep experts say you should do instead.
How Your Body’s Relationship With Melatonin Changes After 50?
At 25, your body produces melatonin like clockwork. By 55, that clock has been quietly losing accuracy for years. Your pineal gland, the tiny structure in your brain that makes melatonin, produces less of it as you age.
Levels that peaked in your teen years drop steadily through adulthood.
By your 50s, your natural output is much lower than it once was. Your circadian rhythm also weakens with age. The internal body clock becomes less precise. That’s why you feel sleepy earlier in the evening and wake earlier than you want to. It’s not a habit. It’s biology.
Your body clears melatonin more slowly after 50. A standard 5 mg dose can stay active in your bloodstream for 12 or more hours. In a younger person, it clears in half that time.
So when you wake at 6 AM feeling foggy and off-balance, that melatonin from the night before is still circulating in your system.
About 40% of adults over 55 report poor sleep quality, according to research published in PMC. For adults over 65, that number climbs to 50, 80%. And here’s a number worth knowing: your body naturally produces only about 0.3 mg of melatonin per night.
Most over-the-counter supplements deliver 10 to 30 times that amount. So if your body is already producing less melatonin and clearing it more slowly, what does it mean when you keep needing more just to fall asleep?
What Does Needing a Higher Dose Actually Tell You?
It’s tempting to think: if some melatonin helps, more must help more. But for adults over 50, that logic can backfire. Immediate-release melatonin peaks in your blood within 30 to 60 minutes, then drops off fast.
If you’re waking at 2 AM, a larger dose of that same formula won’t keep you asleep.
The melatonin is already gone by then. You don’t need more milligrams. You need a different approach.
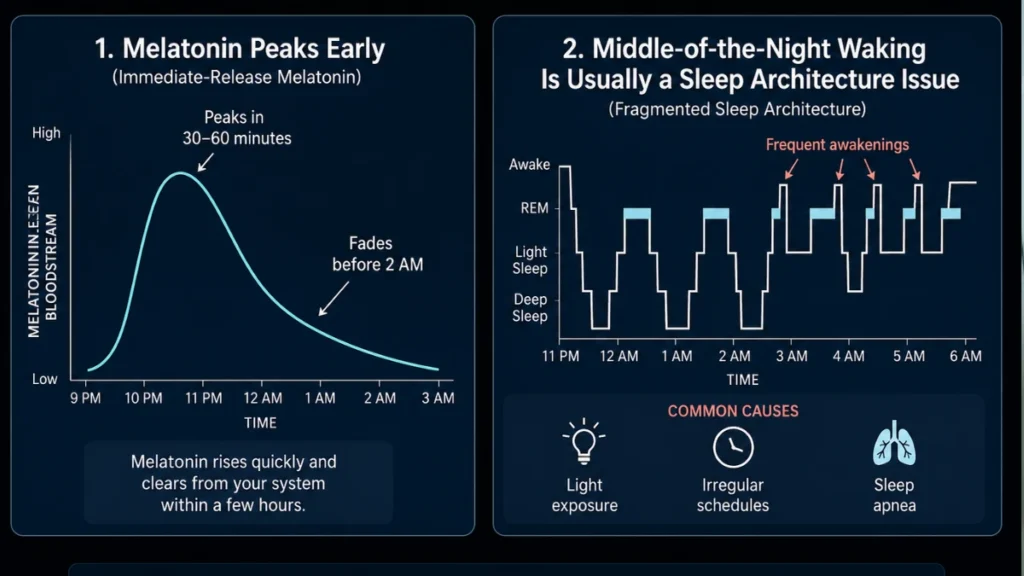
Waking up frequently is usually a sign of fragmented sleep architecture. That’s a pattern tied to things like light exposure, irregular sleep schedules, or underlying conditions like sleep apnea.
It is not simply a melatonin deficiency you can fix by doubling your dose. For women going through menopause or post-menopause, hormonal changes directly affect the circadian system. That makes supplementation more complex, not simpler.
There’s also a dose creep trap. Taking more melatonin to chase better sleep can actually blunt your body’s own production signals over time.
A 2024 meta-analysis in the Journal of Pineal Research found that melatonin benefits peak at around 4 mg per day. Doses above that add no extra sleep benefit but do increase side effect risk.
A large November 2025 study reviewing health records from over 130,000 adults found that long-term melatonin users had higher rates of heart failure and all-cause mortality compared to non-users.
This study is still preliminary and not yet peer-reviewed, so it isn’t the final word. But it is a reason to pay attention.
The Risks of Getting Your Dose Wrong After 50
That groggy, off-balance feeling you have at 7 AM isn’t just unpleasant for adults over 50; it’s a warning sign. Morning grogginess means melatonin is still active in your bloodstream.
For older adults, this directly raises fall risk. Falls are one of the leading causes of injury in this age group.
A 5 mg dose that lingers for 12+ hours can cause dizziness and unsteady movement well into the next morning. Drug interactions are another underappreciated risk. Melatonin interacts with blood thinners like warfarin, antidepressants, beta-blockers, and blood pressure medications, all commonly prescribed to adults over 50.
Beta-blockers alone can suppress your natural melatonin production by up to 50%, which may be why you feel like you need more. There’s also a labeling problem.
A 2023 study in JAMA found that 88% of over-the-counter melatonin gummies were inaccurately labeled.
The actual dose ranged from 74% to 347% of what the package said. So when you think you’re taking 3 mg, you might be taking 10 mg or less than 1 mg. That makes it nearly impossible to manage your dose responsibly without a verified product.
Smarter Melatonin Practices for Adults Over 50
What sleep medicine specialists actually recommend for adults over 50 looks very different from what most pharmacy shelves suggest. Start much lower than you think you need.
Expert guidance in 2025 recommends 0.3 to 1 mg for adults over 50, not the 5 or 10 mg gummies sold at most pharmacies.
The European Food Safety Authority recommends staying at or below 1 mg to get the sleep-onset benefit. More is not better here.
Match the formula to your actual problem. If you have trouble falling asleep, use immediate-release melatonin taken 30 to 60 minutes before bed.
If you wake up in the middle of the night, use a prolonged-release formula instead. It releases melatonin slowly throughout the night, mimicking your body’s natural curve.
The 2 mg prolonged-release version has the most evidence behind it for adults over 55.
Timing matters more than most people realize. Research from the Journal of Pineal Research found that taking melatonin 3 hours before your target bedtime works significantly better than taking it right before sleep.
Don’t forget morning light. Getting outside within 30 to 60 minutes of waking, even on a cloudy day, is one of the most effective ways to reset a drifting circadian rhythm. Aim for 20 to 30 minutes.
Also, look for products marked USP Verified or NSF Certified.
These have been independently tested and are far less likely to have the labeling problems found in other brands. And if adjusting your dose and habits doesn’t bring relief within a few weeks, it’s time to have a different kind of conversation.
When Your Sleep Problem Needs More Than Melatonin
Sometimes the real problem isn’t melatonin at all. Undiagnosed sleep apnea is extremely common in adults over 50, especially in women after menopause, and it’s badly underdiagnosed.
It causes repeated nighttime waking that no amount of melatonin can fix. A home sleep test can screen for it, and it’s worth asking your doctor about.

Cognitive Behavioral Therapy for Insomnia, known as CBT-I, is the treatment the American Academy of Sleep Medicine recommends first, before any medication or supplement. It works on the thought patterns and behaviors that keep insomnia going.
The long-term results are strong, and it addresses root causes rather than masking symptoms. For women in perimenopause or post-menopause, hormonal changes alter the circadian clock itself.
Sleep issues in this context often need targeted management, including possible hormone therapy, CBT-I, and lifestyle changes, not just melatonin adjustments.
If you take beta-blockers, SSRIs, or blood pressure medication, talk to your prescribing doctor. Your medications may already be suppressing your natural melatonin or disrupting your sleep architecture without you knowing it.
See a sleep specialist if your symptoms have lasted more than 3 months.
If you wake gasping or with a racing heart, if you wake with morning headaches, or if a partner has noticed you snore loudly or stop breathing during sleep. These are red flags that go beyond what any supplement can address.
Conclusion
Melatonin after 50 is not a simple math problem. Your body clears it more slowly, produces it less reliably, and responds to it differently than it once did. Taking more is rarely the answer.
Drop to 0.5,1 mg. Switch to prolonged-release if you wake at night. Get 20 minutes of morning light. If nothing improves in 3,4 weeks, see your doctor not for a prescription, but to find the real cause.
Getting your melatonin dose right after 50 isn’t about finding the strongest pill. It’s about listening to what your body is already trying to tell you.
⚠️MEDICAL DISCLAIMER
This article is for informational purposes only. It does not replace medical advice, diagnosis, or treatment. The information covers melatonin production, aging and pineal gland function, circadian rhythm changes, melatonin clearance timeline, sleep architecture fragmentation, light exposure, menopause and sleep, dose-dependent side effects of melatonin, health risks of long-term melatonin use, fall risks and morning grogginess in older adults, supplement drug interactions, supplement labeling accuracy, immediate-release vs. prolonged-release melatonin dosing, morning light exposure, third-party supplement certifications, sleep apnea screening, Cognitive Behavioral Therapy for Insomnia (CBT-I), hormone therapy.
Individual results vary based on age, health status, and fitness level. Before changing your exercise routine, diet, or supplement use, talk to your doctor or a qualified health professional first. If you experience chest pain, dizziness, severe joint pain, or any sudden symptom during or after exercise, stop immediately and seek medical care.